


URGENT: Meta-Analysis from Iranian University Shows Multiple Sclerosis, Neuromyelitis Optica Spectrum Disorder Likely Being Caused by mRNA Injections
Study published 1/17/23 by researchers at Isfahan University of Medical Sciences in Iran

This is a meta-analysis conducted and just released by researchers in Iran on MS and NMSOD — both classified as auto-immune disorders. Caveat that the researchers claim more investigations need to be conducted — these cases are worth drilling into to understand the underlying mechanisms (specifically, T-cells: CD4 & CD8) that are driving some of the neurological disorders.
Why aren’t more investigations being conducted? Maybe there’s no money for such investigations. Or maybe the money is just needed elsewhere, more urgently, in the minds of those who control the purse strings.
Perhaps this is why:

Other cases like this to review:
Full article available here:
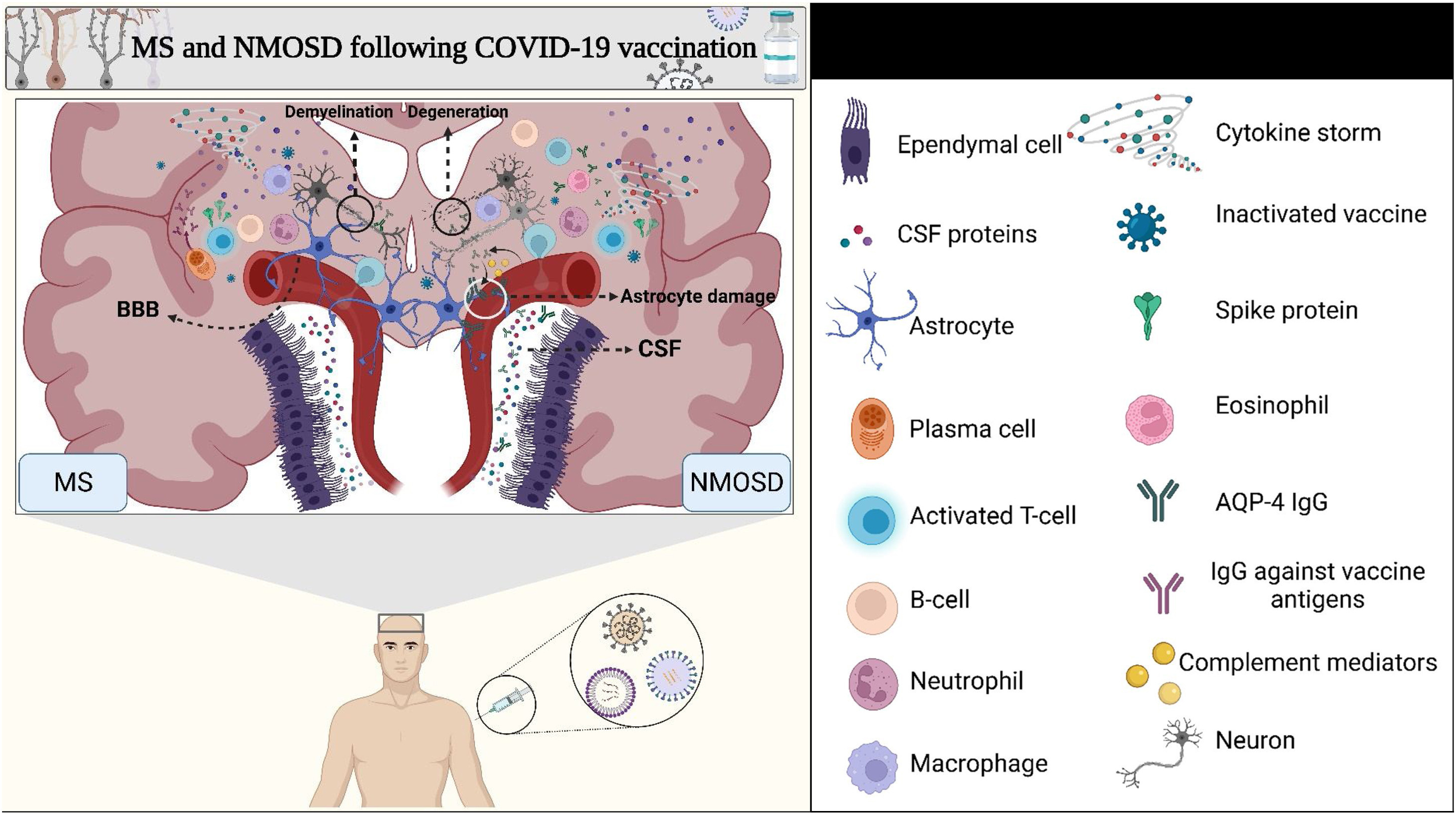
Multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD) following COVID-19 vaccines: A systematic review
Relevant excerpt from the study:
4.4. MS and NMOSD following vaccines injection
There is ample evidence that vaccines may alter the risk of MS.
Within three years after HBV or Human papillomavirus (HPV) vaccination, the risk of CNS demyelinating illness was examined in a case-control study. As a consequence, immunologically induced CNS demyelinating illness was associated with vaccination during the first 30 days of life in younger groups [52]. Vaccines for influenza, diphtheria, tetanus, and pertussis are most commonly associated with a weakened immune system [[52], [91], [92], [93]]. This study concluded that since 3 of 24 individuals had a family history of MS or another systemic autoimmune disorder, the vaccine only accelerated the symptoms of demyelination under pre-existing disease conditions [52].
An investigation conducted in Manitoba, Canada involved 341,347 people vaccinated with Arepanrix H1N1 (AS03-adjuvanted H1N1 pandemic influenza vaccine) during the 2009 pandemic and 485,941 persons who were not vaccinated. The incidence of MS was 17.7 cases per 100,000 person-years in the cohort that had received vaccination and 24.2 cases per 100,000 in the cohort that had not. Also, a hazard ratio of 0.92 was calculated [94]. In conclusion, these studies have shown that vaccination is not only not associated with an increased risk of MS, but rather lower risk of MS. According to a study by Isai et al., GBS was the most common adverse event following flu vaccination, not MS or NMOSD [94]. In the same sense as the Williams et al. study, the most frequent diagnoses associated with the flu vaccine were GBS (37%) and seizure (11%) [66]. According to a case report, the early weeks following H1N1 vaccination are also associated with higher relapse risk in patients with MS [95]. Besides, a randomized trial revealed that the researchers did not find evidence that influenza vaccination leads to an increase in exacerbations in patients with MS post-vaccination or a change in disease course after the vaccination [66].
Human antigens and SARS-CoV-2 molecules can exhibit similar molecular properties, causing autoimmune diseases in those who receive the vaccine [96]. Twenty-one human tissue antigens are cross-reactive with SARS-CoV-2 antibodies. This could explain the cause of autoimmunity resulting from COVID-19 infections and SARS-COV-2 mRNA vaccines affecting the gastrointestinal tract system, cardiovascular system, nervous system, and connective tissues [96]. In addition, mRNA vaccines may trigger a cascade of immune responses that lead to aberrant activation of acquired and innate immunity [97]. Furthermore, certain adjuvants can cause self-reactive T cells to differentiate, causing tissue damage to the host [98]. Activating pattern recognition receptors (PRRs) is one way adjuvants induce innate immunity. It is for this reason that vaccines contain them in order to stimulate the production of immunity against antigens [99]. Compared to previous vaccines, SARS-CoV-2 adjuvanticity acts as an agonist for TLR-7/8 or TLR-9. There is a possibility that this is a new pathogenic mechanism responsible for human immune-mediated diseases [100]. Meanwhile, the activation of adaptive immunity in response to vaccines is also governed by TLR pathways. As a result of these findings, it is evident that TLRs play a significant role in vaccine efficacy as well as the pathogenesis of MS and NMOSD [[101], [102]].
In the case described by Chen et al., the female patient presented with symptoms of weakness 3 days after the first dose of an inactivated COVID-19 vaccine and was diagnosed with NMOSD following performing MRIs and observation of area postrema and bilateral hypothalamus lesions without gadolinium enhancement [41]. This may be because, following increasing the permeability of the BBB, molecular mimicry is performed by the vaccine (as in the SARS-CoV-2), and triggering the immune cells leads to inflammation, and eventually, NMOSD occurs. According to another study by Fujimori et al., a patient with a prior inflammatory background in CNS following mRNA COVID-19 vaccine injection developed MS [35]. Notably, this subject previously had a brain lesion, uptook steroids, and there was an appropriate environment to contract other neurological disorders in her CNS. A case reported by Caliskan et al. developed NMOSD one day after the second dose of an mRNA COVID-19 vaccine [45]. An issue that needs to be addressed is the pre-vaccine titer of the AQP4 antibody. This is because the person may have a high antibody titer before the vaccine and be prone to developing autoimmunity. All these factors must be investigated for a definite statement that vaccination may trigger MS or NMOSD, but until then, the cause-and-effect relationship is unclear.
In this systematic review, we comprehensively assessed all case reports on MS and NMOSD patients following COVID-19 vaccination with various platforms. Although this is the first systematic review in this regard, we had some limitations composed of the low number of cases which shows it is not able to represent the population and the lack of available data for all vaccines.
Abstract:
Background: The global COVID-19 pandemic began in March 2019, and given the number of casualties and adverse effects on the economy, society, and all aspects of the health system, efforts have been made to develop vaccines from the beginning of the pandemic. Numerous vaccines against COVID-19 infection have been developed in several technologies and have spread rapidly. There have been reported multiple complications of the COVID-19 vaccines as with other vaccines. A number of studies have reported multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD) as complications of COVID-19 vaccines.
Methods: First, we found 954 studies from 4 databases (PubMed, Embase, Scopus, and Web of Science) from inception to March 1st, 2022. Next, duplicate articles were eliminated, and 476 studies remained. Then 412 studies were removed according to inclusion and exclusion criteria. After obtaining the full text of 64 articles, 12 studies were selected finally.
Results: The data were extracted from included studies in a table. Our data includes demographic data, comorbidities, vaccines information and side effects, NMOSD and MS symptoms, laboratory and cerebrospinal fluid (CSF) findings, magnetic resonance imaging (MRI) results, treatment, and outcome of all cases.
Conclusion: MS and NMOSD are two neuroinflammatory disorders that arise in the CNS. Cases of MS and NMOSD have been reported following COVID-19 vaccination. Nevertheless, more studies with more subjects are needed to assess any possible relationship between the COVID-19 vaccine and central nervous system demyelination.
Similar reading:
Concluding with plausible solutions to these problems & others:
Wow. I wonder if a lot of the clusters of side effect profiles we are seeing are MS.